The Physician Gender Pay Gap is $0.78 on the Dollar. Adjust for Everything, and it's Still $0.93.
Today marks Equal Pay Day 2026, a stark reminder that men continue to out-earn women across the U.S. workforce. According to new Marit research, women in medicine are no exception. In addition to female physicians, who earn just $0.78 for every dollar men earn, physician assistants (PAs), nurse practitioners (NPs), and certified registered nurse anesthetists (CRNAs) all report lower pay than their male peers according to more than 15,000 of anonymized salaries shared on Marit.
For female physicians, the pay gap adds up to $3.3 million in lost lifetime earnings over a 30-year career. Compensation in medicine is influenced by several factors, including specialty, experience, type of employer, compensation structure, workloads and geography. Even after accounting for a wide variety of these factors, we still see an unexplained pay gap of 2% across roles. In other words, all the typical explanations for why male healthcare providers tend to earn more than women do not fully explain the gap in earnings.
With healthcare facing ongoing workforce shortages and burnout, closing the gap is not only about equity - it is critical to retention.
Men outearn women across medicine
The gap in reported total compensation is widest among physicians, where women earn $0.78 on the dollar compared to their male peers. Total compensation among female PAs ($0.96), NPs ($0.96) and CRNAs ($0.94) is much closer to their male peers, though they make up 75% of the the workforce for these professions.
Though there has been some progress toward gender parity in the workforce, there remain sharp divides in gender representation among clinicians: Under 40% of all physicians are women, while roughly 75% of PAs and NPs are female. Among CRNAs there is a somewhat more even gender balance, with women accounting for about 57% of clinicians.
.png)
Specialty is associated with about half of the pay gap among physicians, and about a third of the gap among nurse practitioners
Specialty area is the single largest factor associated with the pay gap among physicians – accounting for about $0.11 of the difference in total compensation between men and women.
Women tend to be underrepresented among physicians in the most lucrative medical specialties – notably neurosurgery, orthopedic surgery, cardiology and radiology where experienced physicians routinely earn more than $600,000 annually in total compensation but where less than one-in-five physicians is female.

Women choose less intensive schedules that impact pay
Healthcare employers pay practitioners more for roles that require intensive or nonstandard work schedules – for instance long shifts, weekend or variable schedules, or frequent on calls. Across all four professions, females are less likely to work nonstandard or intensive schedules. For example, Male physicians are 18.3% more likely to report having a high on-call burden, defined as being on call every two days or more. Further, 44% of male PAs work weekend or variable schedules, compared to 35% of female PAs. Among NPs, 25% of females report working long or variable hour days (i.e., shifts that are 12 hours or longer, or are variable) compared to 35% of male NPs. Female CRNAs are more likely to have a low on call burden: 63.8% of female CRNAs compared to 62.3% of male CRNAs report a low on call burden.
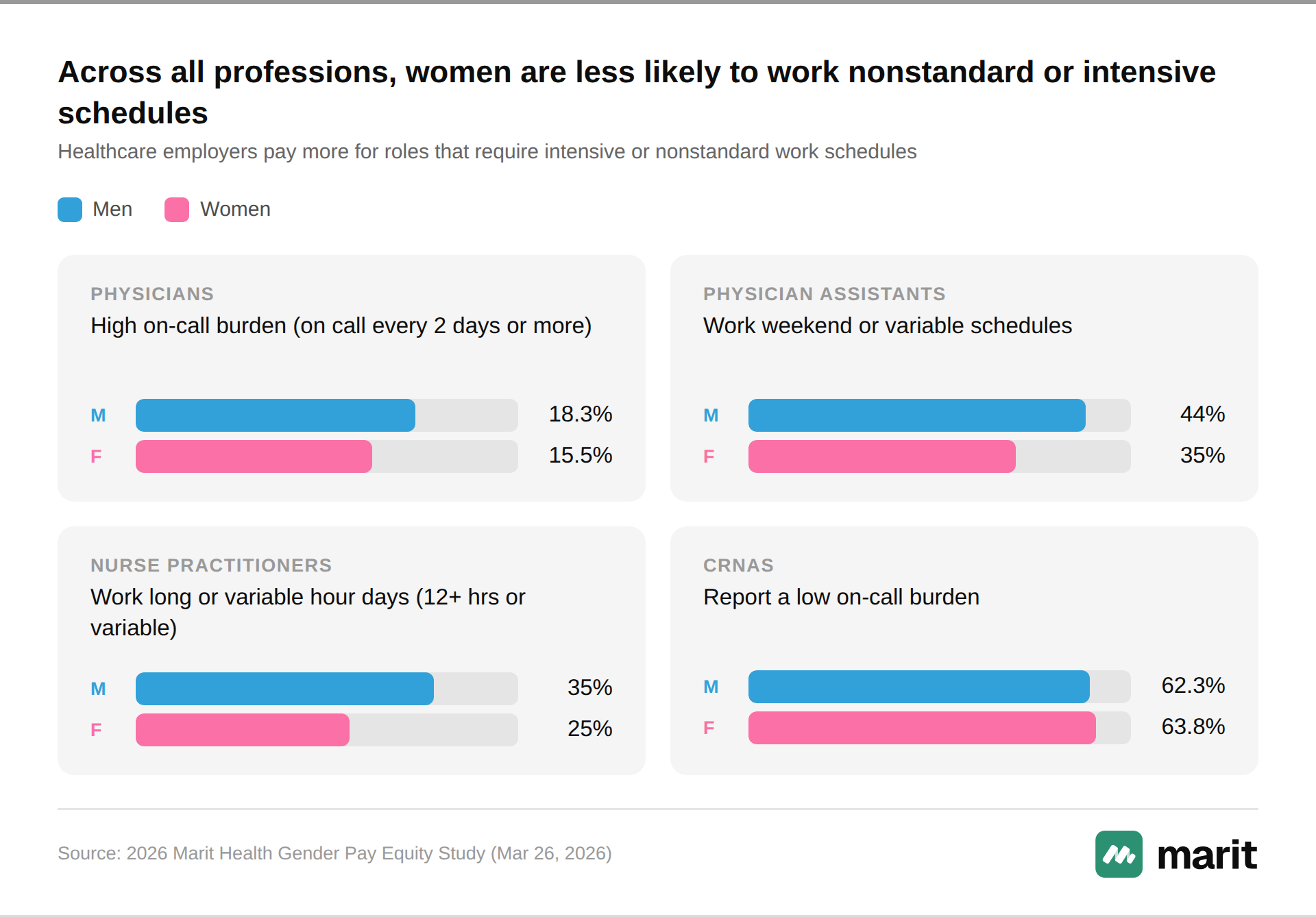
Work-life requirements are a common barrier to females across the labor force, but are particularly important in healthcare where intensive workloads are common in the most lucrative niches.
Women are more likely to work in the public or non-profit sector where pay tends to be lower
Female physicians, NPs and CRNAs are more likely than males to work in the public or nonprofit sector.
- 6.9% of female physicians work at a Federally Qualified Health Center (FQHC), a nonprofit organization, or for a government entity compared to 4.8% of male physicians.
- 4.8% of female CRNAs work at a FQHC, a nonprofit organization, or for a government entity compared to 2.6% of male CRNAs.
- 9.6% of female NPs work at a FQHC, a nonprofit organization, or for a government entity compared to 7.5% of male physicians.
Physician assistants are an exception to this pattern: 6.6% of male PAs work at FQHC, a nonprofit organization, or a government entity compared to 5.6% of female PAs.
Men are more likely to report incentive pay across all professions, and among those who report any, it is a higher portion of total pay
- For physicians, PAs, NPs and CRNAs, males are more likely to report receiving any incentive compensation
- Among professionals who report any incentive pay, it generally accounts for a larger share of total compensation for males than for females. The one exception is among PAs.
.png)
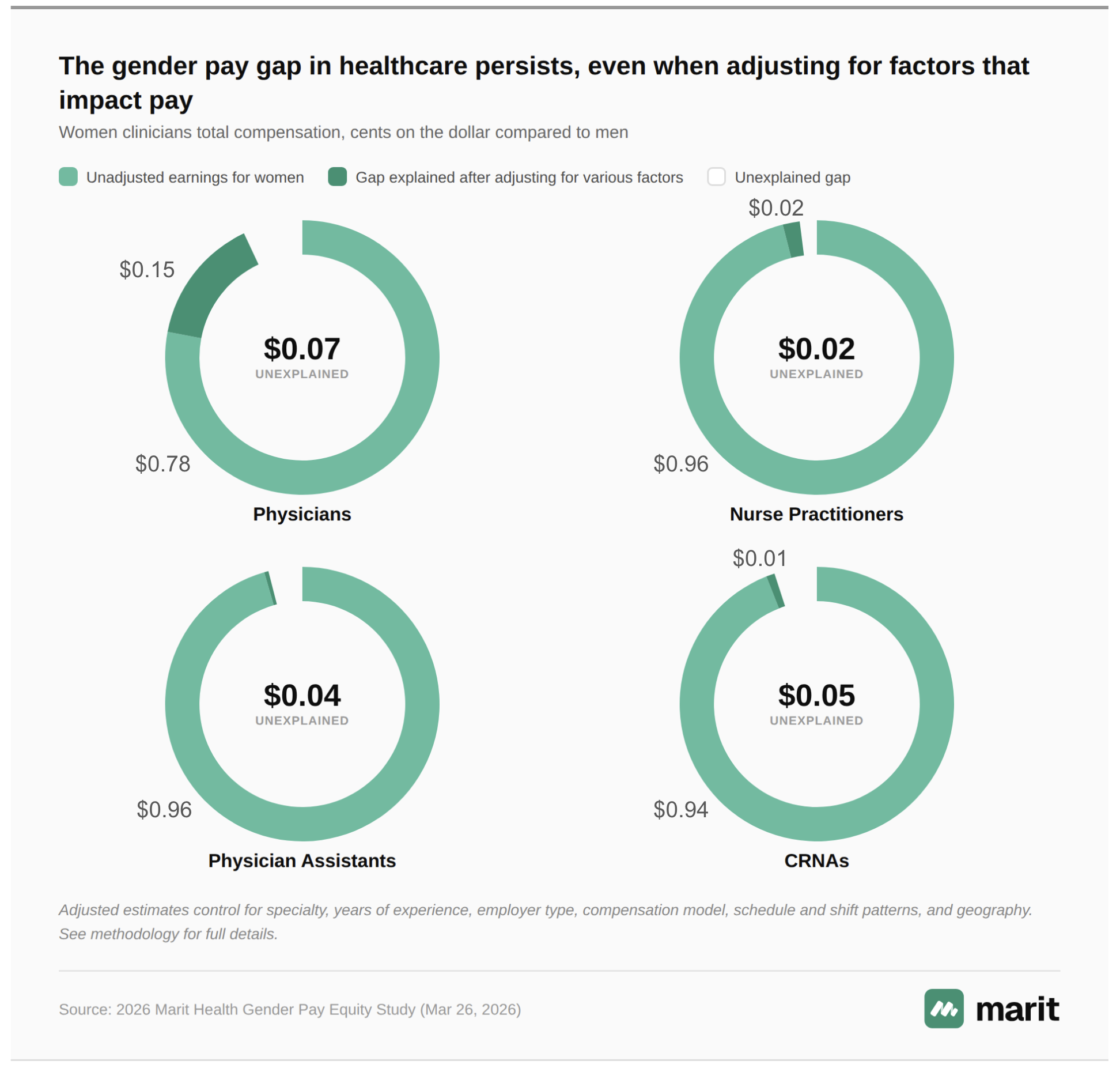
After adjusting for these differences, female medical professionals continue to earn $0.98 to $0.93 on the dollar compared to their male peers
Adjusting for a wide range of pay-relevant variables – including specialty, years of experience, workloads, employer type, compensation structure and geography – male medical professionals continue to out-earn their female peers, though the margin is generally narrower than the unadjusted gap.
- Among physicians, the factors are associated with about two-thirds of the gender pay gap. Adjusting for them narrows the difference in total compensation between men and women, but women still continue to earn about $0.93 on the dollar.
- Among NPs, these factors are associated with about half of the pay gap between men and women – narrowing the difference in total compensation to $0.98 on the dollar.
- Among CRNAs, these factors are associated with about one-sixth of the raw gap in total compensation, with female CRNAs earning $0.95 on the dollar.
- Among PAs, these factors tend to move in opposite directions – for instance, female PAs tend to be more experienced (and thus better paid) than male PAs, but also work in less lucrative specialty areas. Adjusting for these factors on net does not change the gap in total compensation: Female PAs still earn $0.96 on the dollar compared to their male peers
Closing the gender pay gap starts with transparency
Closing the gender pay gap in medicine is not just about equity. It's about the future of healthcare. When women in medicine are systematically underpaid, they burn out faster, leave practice earlier and step back from leadership. In a country already facing a clinician shortage, equal pay for equal work helps to drive better outcomes for everyone – the clinicians and patients.
For too long, compensation in medicine has been a black box hidden behind expensive paid subscriptions. Closing the pay gap in medicine requires equal access to information. Marit Health was built on this core belief – that more transparency about pay leads to increased pay equity.
Share your anonymous salary with the Marit community – the largest peer-reported physician compensation dataset in medicine, with more than 23,500 submissions. It is free, physician-led and completely anonymous (even for smaller specialties).
Compare your salary with other anonymous salaries across all dimensions (base, bonuses, workload, schedule, benefits, and more). You can also access the latest 2025 MGMA benchmarks on Marit completely free. Use this to advocate for yourseld. Let's close this gap together.
Methodology
The results are based on 15,151 anonymous pay reports submitted to Marit Health for medical specialties through March 18th, 2026: 10,865 from physicians, 2,766 from PAs, 1,260 from NPs, and 260 from CRNAs. It includes only practicing professionals who reported working full time. All salary submissions are moderated using a combination of algorithmic and human moderation to ensure data accuracy. All survey respondents are asked to claim their NPI at the end of the survey to ensure submissions are for NPI verified professionals only. Sex data was obtained from the CMS NPI Registry through an NPI lookup from the survey.
We regress log total compensation and base salary as a function of five sets of controls:
- Years of experience, binned
- Specialty
- Employer and compensation model: Employer type, compensation model, whether the individual reported leadership responsibilities, and the incentive pay share of total compensation
- Schedule and shifts: Scheduled hours and days
- Location: cost of living, metropolitan status, and region
Additional controls were included in the analysis of physician compensation.

Let's close the gender pay gap